TMJ Explained
TMJ Definition and Components
TMJ (temporomandibular joint) dysfunction, sometimes labeled TMD, is a disharmony between the way the jaw joint works in its most unstrained position and the way the teeth occlude during those movements. There can be many causes of this disharmony. Some possible causes of this disharmony include tooth loss, restorative dentistry without properly adjusted occlusion, accidents (like whiplash), mal-positioned and/or underdeveloped cranial or jawbones, and perhaps habits like clenching or grinding the teeth. For optimal TMJ health to exist, there must be a harmony between the way the mandibular (lower jaw) condyle is positioned in the glenoid fossa (joint space) and the way the upper and lower teeth occlude (come together). If this harmony does not exist, one or more of four conditions will develop. There could be:
- excessive wear patterns on the teeth
- fracturing of the teeth
- loosening of the some or all of the teeth
- development of any or all of the TMJ dysfunction symptoms explained elsewhere in this website.
Often we will be able to recognize one or more of the first three above mentioned conditions prior to the onset of TMJ dysfunction symptoms and take steps to prevent their occurrence.
There are always two components to the temporomandibular joint dysfunction: a structural component and a stress component.
The Structural Component
The lower jaw is sort of in a sling of muscle and tendons whose job it is, in addition to opening and closing the mouth, is to position the lower jaw where ever it needs to be in order to get maximum interdigitation of the teeth. If the upper jaw (maxilla) is shifted to one side, canted up on one side, slanted (one side farther forward than the other), sloped too steeply, positioned too far forward or backward, or too high or too low, then the muscles and tendons of the lower jaw (mandible) have to move it into an eccentric and strained position for the teeth of the two jaws to come together optimally. Because of the way many nerves and blood vessels exit the skull in the area of the temporomandibular joint, this eccentric position of the lower jaw can impinge on them setting up the conditions leading to the myriad of symptoms stated elsewhere at this website.
A second structural problem, and a very common one indeed, is the loss of vertical dimension. This could be thought of as the "chin-to-nose" distance. The ideal vertical dimension can be compromised any number of ways: collapse of the dental arch due to the loss of one or more teeth; excessive wear of the teeth; orthodontic extractions; an arch size discrepancy between the upper and lower dental arch; or possibly a genetic predisposition. At any rate, this hyperflexion of the jaw joint puts pressure on the nerves and blood vessels, which exit the skull through the joint space, thereby precipitating the one or more of the symptoms associated with TMJ dysfunction.
The Stress Component
There is also a stress component to TMJ dysfunction. Actually, neurological pathways have now been identified and defined, which explain the relationship of stress to TMJ dysfunction. Often, there is a feeling of hopelessness and/or helplessness, which goes along with full-blown TMJ cases. A state of depression is a common finding. It is hard to identify which came first, "the chicken or the egg." Did the pain and frustration of not finding someone who could help cause the depression, or did the depression precipitate the TMJ symptoms.
In fact, in some instances, the symptoms of TMJ will be significantly reduced simply by removing known stressors. Because in our fast-paced society there are so many stressors, it is often difficult, if not impossible to eliminate them. A more practical approach is to learn to entrain our sympathetic and parasympathetic nervous systems at will, so that the stressors don't have the disasterous effects on our body organs and immune system. This, in fact, can be accomplished and the benefits are quite remarkable. The technique can be learned quickly.
Function of the TMJ
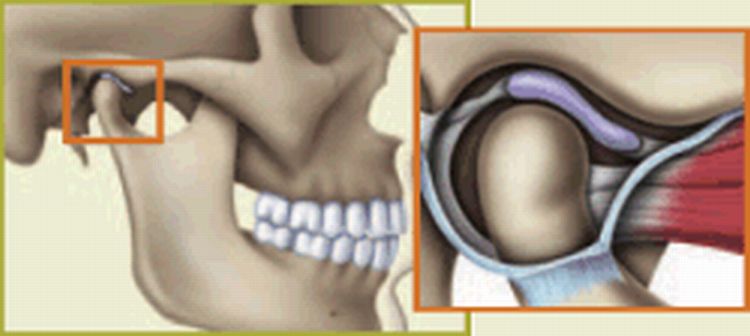
Temporomandibular joint — Normal closed position. Jawbone is separated from skull by a soft disk that acts as a cushion when you chew, speak or swallow.
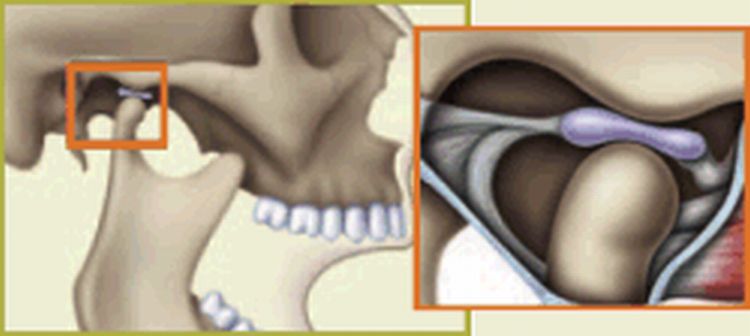
Temporomandibular joint — Noraml open position. Disk stays in place when jaw is in use.
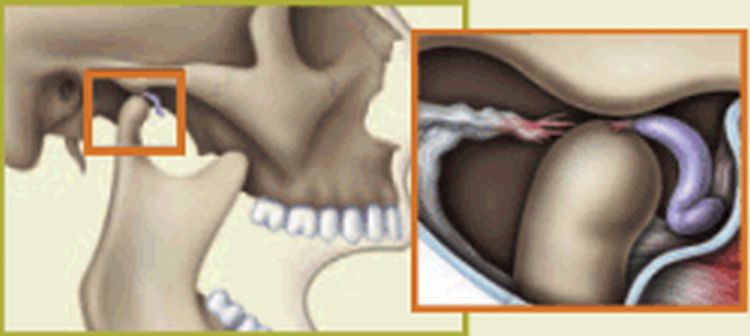
Temporomandibular joint — Abnormal. Disk is pulled forward when jaw is in use, causing the bone structures to grind together.
Symptoms of TMJ Dysfunction
The symptoms of TMJ dysfunction are unbelievably diverse, both in nature and in severity. The most common symptoms are migraine-like headaches, which seem to come from behind the eyes or the side of the head. Also, there are the headaches or neckaches, which occur at the back of the head right where the neck attaches to the skull. People usually describe these neckaches as "tension headaches", as they are often associated with stress. The pain often radiates down into one or both shoulders. Another type of headache associated with TMJ dysfunction may occur in the area of the cheekbones, resembling a "sinus headache." Still other types of TMJ headaches are those which occur right in the top of the head, or in the area of the jaw joint, or fan out over the side of the head. These types may be either continuous or sort of come in waves.
Slightly less frequent, but occasionally more severe symptoms include vertigo (dizziness), ringing in the ears, lancing pain in one or both ears or in the jaw joint itself, hearing difficulties, stuffiness in one or both ears, light sensitivity in the eyes, ulcer-like pains in the stomach, low back pain, and poor posture. Occasionally there will even be tingling or numbness in the fingertips of one or both hands.
More obvious, but less severe TMJ symptoms include clicking, popping, and/or grinding (crepitus) in the jaw joint; tenderness or pain in the jaw joint; sore or painful muscles in the head, face, or neck; difficulty in chewing; fatigue of the jaw muscles after prolonged chewing or talking; limitations of the range of motion of the lower jaw; locking of the jaw in either the open or closed position; clenching or grinding the teeth; sensitivity of the teeth; nibbling or chewing on the inside of the cheek; and deviation of the jaw when opening or closing the mouth.
Treatment of TMJ Dysfunction
Occlusal Adjustment
Rarely, it will be found, after a thorough evaluation, that a single tooth or a very few teeth are causing interferences which precipitate TMJ dysfunction. It can be a rotated tooth, a mal-posed tooth, a mal-formed tooth or a number of other possibilities. Provided it has been shown through the records process, that all the other criteria are within the range of physiological adaptation, then "spot grinding" of one or a very few teeth may be the indicated treatment. Discernment must be used in order to know which tooth to grind, so that relieving one interferences does not create a new one in a different place.
Occlusal Equilibration
Somewhat more frequently, it will be found after a thorough evaluation, that orthopedically, everything is within normal limits, but a good number of teeth just don't function well together. In this case, the treatment of choice may be to do an occlusal equilibration of the entire mouth. However, this should always be performed first on stone models of the mouth, which have been mounted on a properly programmed articulator so that the correct teeth and the precise areas of adjustment can be determined. In this way, the dentist knows before hand, not only where and how much tooth structure will have to be removed, but also, exactly what the resulting function of the occlusion will be after the equilibration.
Occlusal Splint Therapy
This form of treatment is directed toward symptoms only and rarely, if ever, is directed toward the cause of the TMJ dysfunction. As such, its primary use should be to get symptomatic relief right away in very acute TMJ cases just until proper diagnosis and treatment can be begun. Occasionally, an occlusal splint may be used to assist in the diagnosis when both the symptoms are vague or don't fit the clinical pattern and the diagnostic findings are not conclusive. In those cases, a substantial reduction of symptoms from the use of the splint may confirm the diagnosis of TMJ dysfunction.
Surgery
Surgery is an option that is rarely indicated for TMJ dysfunction. As a rule, it should be considered only as a last resort. If there has been an accident where the jaws have been fractured, then surgery is often indicated. Rarely, there will be a "bone spur" or some other anomaly of the bone, which can only be corrected surgically.
My experience has been that rarely, in the case of TMJ dysfunction, has surgical joint replacement or disc replacement resulted in a satisfactory condition. Occasionally, like the television shows have demonstrated, the results have been total nightmares for everyone involved.
Full Mouth Reconstruction
Sometimes cases present in which all the orthopedic and orthodontic records are within normal limits and the normal physiological adaptive range, but the teeth have worn excessively or for some other reason have lost vertical dimension. Loss of vertical dimension is one of the most important factors in TMJ dysfunction and it must be restored for optimal health to exist. Sometimes, the only and/or best way to acquire adequate vertical dimension is by placing crowns on all the teeth or occasionally only the posterior teeth.
Again in this instance, it is mandatory that before any teeth are prepared for crowns, a diagnostic wax-up is done on accurate dental models properly mounted on a programmable articulator. This must be done so that the final result can be visualized and examined prior to any irreversible changes have been made to the actual tooth structure.
Also, extreme attention to detail must be placed on the esthetics of the finished case, and care must be taken to make sure that the phonetics of the finished case is ideal. In other words, it is not acceptable for the patient to hiss or whistle when making "s" sounds in their normal speech. Also, extreme care must be taken to allow the "f" and "v" sounds to be normal and comfortable for the patient to make.
Cranial-Mandibular-Cervical (CMC) Orthodontics
CMC orthodontics is next generation of what is sometimes called gnathologic orthopedics or orthopedic gnathology or orthopedic orthodontics. It is the most advanced and comprehensive form of treatment on the planet for TMJ dysfunction and orthodontic correction. The differences between CMC orthodontics and traditional orthodontics are extensive. The initial phase of CMC orthodontics is devoted to getting the bones of the jaws and the skull in their proper position and in an orthogonal (right angle) relationship with each other. Rarely, if ever, are permanent teeth removed in CMC orthodontics, and the use of "headgear" is virtually non-existent. Additionally, many cases which are considered "surgical cases" can be treated very nicely in a non-surgical manner and with a superior result. Although, CMC orthodontics is generally a two-phase treatment (orthopedic and orthodontic), rarely is total treatment time longer than that of traditional orthodontics. The only exception to this would be when the treatment objective is one, which is completely unobtainable through traditional orthodontics.
Body structures are in a dynamic position. That position is such as it is because that is where all the forces which come into play are in equilibrium. All we have to do to effect the movement and or remodeling of the bone is to very lightly tip the balance of forces in favor of a more ideal or "correct position" for the bones of the skull and the entire masticatory system. Once movement and/or remodeling have begun, we orchestrate the movement of the bones into optimal relationships with each other and that results in a degree of function and comfort that is otherwise impossible to achieve.